1st Dose Consent 2nd Dose Consent INFORMED CONSENT FOR COVID-19 VACCINE 876-002-V10 04192021 FAX COMPLETED PAGE 1 TO. Or c legally authorized to consent for vaccination for the patient named above.
 Covid 19 Vaccine Screening And Consent Form Screening And Consent Form Covid 19 Vaccine Six Nations Covid 19
Covid 19 Vaccine Screening And Consent Form Screening And Consent Form Covid 19 Vaccine Six Nations Covid 19
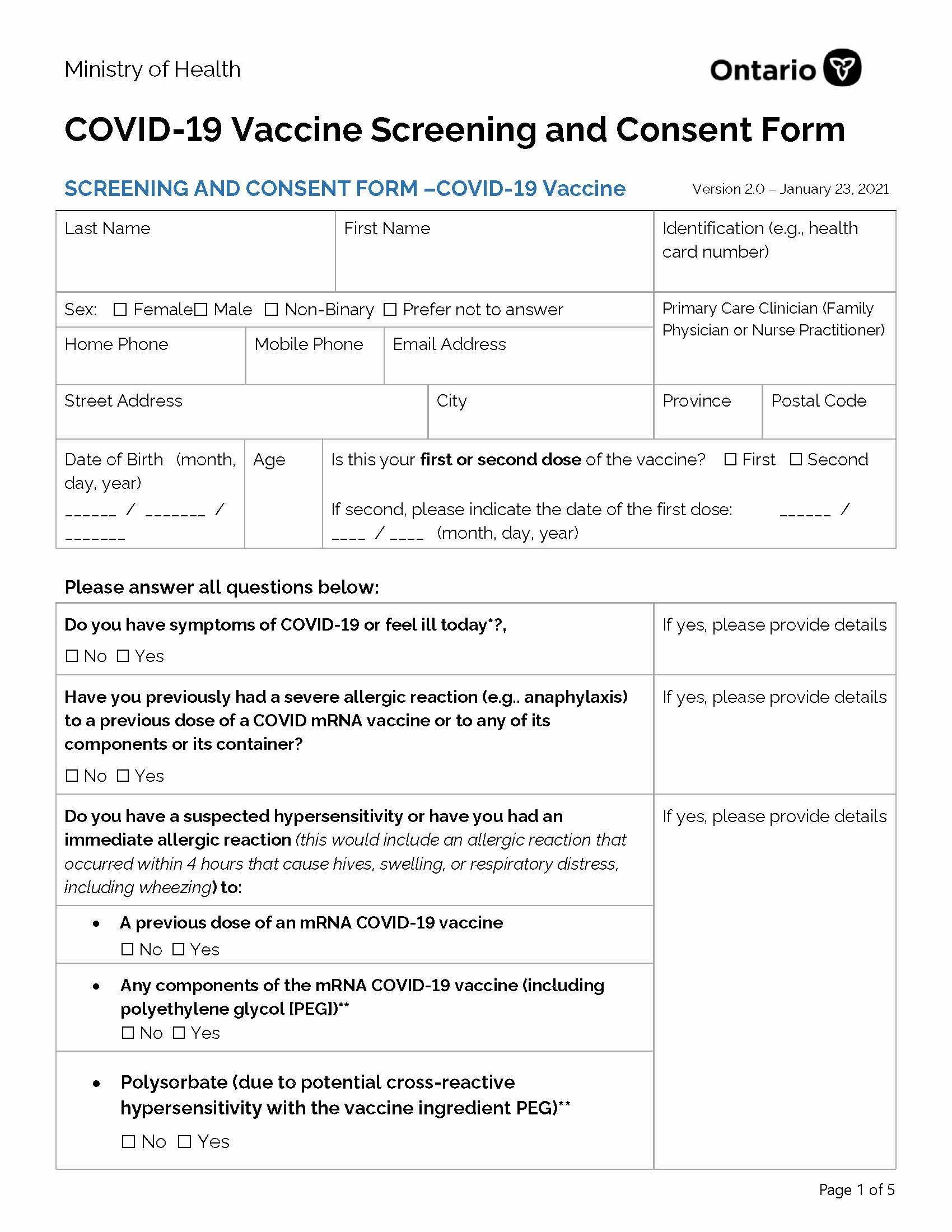
Last Name First Name Identification eg health card number Sex.

Vaccine consent form. The personal health information on this form is being collected for the purpose of providing care to you and creating an immunization record for you and because it. Further I hereby give my con-sent to Hedges Health Mart Pharmacy or its agents to administer the OVID-19 vaccine. Female Male Non-Binary Prefer not to answer.
Consent to Administer the COVID-19 Vaccine Ihave read orhave had explained to me the Emergency Use Authorization EUAfor administration of the COVID-19 vaccine. States law by signing below I hereby do consent to the applicable Provider reporting my vaccination information to the State HIE or through the State HIE andor State Registry to the entities and for the purposes described in this Informed Consent form. Download COVID-19 vaccination Consent form for COVID-19 vaccination as Word- 284 KB 4 pages.
COVID-19 vaccination Consent form Print-friendly. COVID-19 Vaccine Screening and Consent Form. Primary Care Clinician Family Physician or Nurse.
Further I hereby give my consent to the Florida Department of Health DOH or its agents to administer the COVID-19 vaccine. Date of Birth _____. You choose to have the vaccination or not.
When making the appointment it should tell you what vaccine you will be receiving either the Pfizer or the Moderna vaccine then download the form for that particular vaccine. COVID-19 Screening Questions Yes No 1. Version 30 March 11 2021.
The coronavirus COVID-19 vaccination consent form and letter templates are available in different software versions and can be downloaded. Email address Phone Number. Consent will give the designated individual authority to administer the COVID-19 Vaccine.
All of my questions concerning the vaccine have been answered to my satisfaction. I am an adult who can legally consent for the person named below to receive the COVID-19 vaccine. Address City State Zip.
Acknowledgement of Collection Use and Disclosure of Personal Health Information. COVID-19 Vaccine Consent Form. The COVID-19 vaccination is free.
CONSENT FORM COVID-19 Vaccine. Informed Consent Consult immunizer if no signature can be obtained I have read and understood the fact sheets regarding the risks and benefits of the vaccine that I am consenting be administered to the above named person as per section A. COVID-19 VACCINE PARENTAL CONSENT FORM.
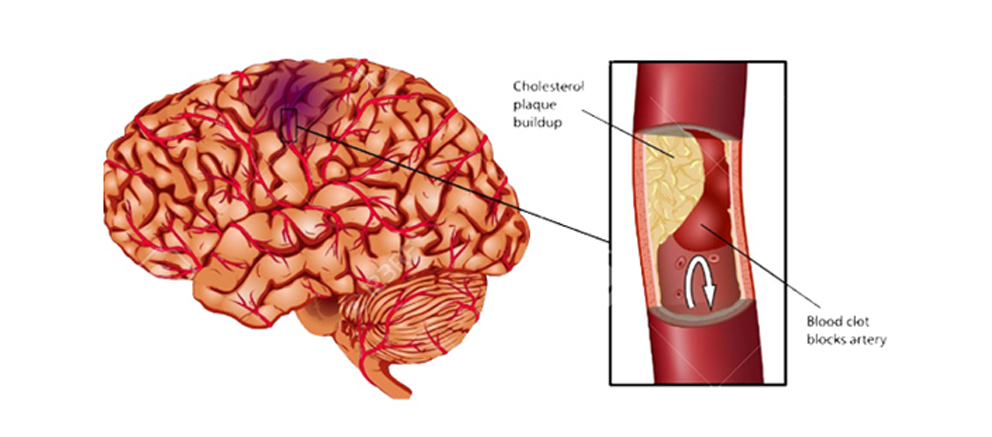
Last Name First Name Date of Birth Gender. We aim to provide documents in an accessible format. The COVID-19 disease that the COVID-19 vaccine is meant to prevent.
Least 16 years of age. I understand that this product has not been approved or licensed by FDA but has been authorized for emergency use by FDA un-. Version 10 December 30 2020.
I freely and voluntarily give my signed consent and permission for the administration and injection of the COVID-19 vaccine. Be ready to present your ID insurance cards and consent form. You need to have the vaccination two times.
COVID Vaccine Intake Consent Form. Female Male Prefer not to answer Other. Is this the first First Middle.
Download COVID-19 vaccination Consent form for COVID-19 vaccination as PDF- 221 KB 4 pages. I consent to receiving the vaccine. I ____ the parentguardian of _____ date of birth ____ __ have received the Emergency Use Authorization for the Pfizer Covid-19 Vaccine and grant consent for my.
Skyline Pharmacy Clinic is offering the Johnson Vaccine for 18 years of age and older. Signed parental consent is required before anyone under the age of 18 will be vaccinated. My consent applies to all doses of the vaccine necessary to complete the series up to one year.
Administration Facility NameFacility ID. _____ Primary Care Clinician Family Physician or Nurse Practitioner If Indigenous please indicate which Indigenous identity. Last Name First Name Identification eg health card number Gender.
I have been given the opportunity to ask a health care professional questions concerning the vaccine. Consent form for COVID-19 vaccination About COVID-19 vaccination People who have a COVID-19 vaccination have a much lower chance of getting sick from the disease called COVID-19. If youre having problems using a document with.
SCREENING AND CONSENT FORM COVID-19 Vaccine. Please complete this form and. To be vaccinated you will get a needle in your arm.
By my signature below I consent to the administration of the vaccines by a pharmacist or a supervised student pharmacist or technician or other authorized person where permitted by law or statefederal guidance employed or contracted by Albertsons Companies or one of its affiliated pharmacies and to be contacted at the number provided. Years of age. COVID-19 Vaccine Consent Form OrganizationFacility Name.
Or c legally authorized to consent for vaccination for the patient named above. The pause for the Janssen vaccine has been lifted and they have updated their fact sheet to include appropiate warnings. View COVID Consent 1pdf from SCIENCE 2 at Veterans High School.
800-447-7167 Page 1 of 2 SECTION A USE BLACK INK PRINT NEATLY VACCINE RECIPIENT INFO. In the past two weeks have you tested positive for COVID 19 or are you.
 8 Home Remedies To Get Rid Of Pubic Lice Fast Pubic Lice Treatment
8 Home Remedies To Get Rid Of Pubic Lice Fast Pubic Lice Treatment 






:max_bytes(150000):strip_icc()/what-is-sputum-22491921-43f5d3e90e9e4eec9613c4a8ca209120.png)